The Problem
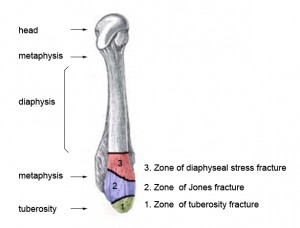
Fifth metatarsal fractures are a common fracture occurring in both children and athletes [1]. While there are inconsistencies in the description of fracture types of the fifth metatarsal, proximal fractures are typically broken up into three zones. Zone one is known as a tuberosity fracture, zone two, Jones fracture, and zone three as diaphyseal stress fractures [2] which can be seen in Figure 1. Fractures of the 5th metatarsal distal to zone 3 typically heal with immobilization of the member. However, fractures at the proximal end of the bone can experience a delayed or nonunion without surgical intervention. In a meta study it was found that non-operatively treated acute fractures had a union rate of 76% while fractures treated with screw fixation acquired union 96% of the time. Delayed unions treated non-operatively versus surgically had union rates of 44% and 97% respectively [3]. The issue of nonunion or delayed union is a serious concern for elite athletes who need to be able to return to high levels of activity in as short of time as possible.
Current Solution and Issues

Stabilization of Jones fractures are commonly done with intramedullary screw fixation which can be seen in Figure 2. This procedure is typically done with a localized anesthesia, where the screw is aligned using a guide wire and multiple radiographic images. While this procedure can alleviate the issues associated with delayed and nonunion it is not without complications. Particularly in athletes, even after surgical intervention of Jones fracture and proper healing time refracture can occur as well as the breaking of the intramedullary screw. Other known issues include the screws breaking out of the bone due to oversizing of the screw [3] [4].
Another method for adjoining proximal fractures is using plate fixation. The plate runs parallel with the metatarsal with multiple fasteners which are inserted transversely through the bone shaft. While the plate method has been used clinically, there is significantly less literature available concerning the use of a plate method for fracture fixation. The question has thus been raised as to which method works better for fixation of proximal fractures of the 5th metatarsal.
Testing

Researchers in the Biomechanical Environments Laboratory are working with orthopedic surgeons at Houston Methodist Orthopedics and Sports Medicine Research Group to determine whether the intramedullary screw or the plate construct is ideal to minimize plantar gap formation and potentially minimize delayed union or nonunion. Testing will be performed on 5th metatarsal cadaver specimens which will have all soft tissue removed prior to testing. A simulated zone 2 (Jones) fracture will be created by the surgeons and then fixed with either the intramedullary screw or plate construct. The repaired specimen will then be setup in a cantilever loading scenario in which a cyclical loading will be applied. The overall amplitude of the cyclical loading will be increased at predetermined points during the testing. This is to better simulate the fatigue based loading the foot receives as opposed to a simple linear ramp up loading. The increase in amplitude is necessary to reach loads similar to those that might be seen in the food during athletic activities.
Research results will be directly relayed to collaborating Sports Medicine Clinicians to buttress the choice of fixation methodologies, which will be used on an impending surgical case and for future reference.
References
[1] S. Raikin, N. Slenker and B. Ratigan, “The association of a varus hindfoot and fracture of the fifth metatarsal metaphyseal-diaphyseal junction: the Jones fracture,” Am J Sports Med, vol. 36, pp. 1367-72, 2008.
[2] L. SJ and B. MJ, “Jones fractures and related fractures of the proximal fifth metatarsal,” Foot & Ankle International, vol. 14, pp. 358-65, 1993.
[3] A. J. Roche and J. D. F. Calder, “Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review,” Knee Surg Sports Traumatol Arthrosc, vol. 21, pp. 1307-1315, 2013.
[4] J. D. Granata, G. C. Berlet, T. M. Philbin, G. Jones, C. C. Kaeding and K. S. Peterson, “Failed Surgical Management of Acute Proximal Fith Metatarsal (Jones) Fractures A Retrospective Case Series and Literature Review,” Foot & Ankle Specialist , 2015.
[5] K. J. Hunt and R. B. Anderson, “Fifth Metatarsal Fractures and Refractures,” Oper Tech Sports Med, vol. 22, pp. 305-312, 2014.
[6] “Wikiradiography-Fifth Metatarsal Fractures,” [Online]. Available: http://www.wikiradiography.net/page/Fifth+Metatarsal+Fractures. [Accessed 12 December 2015].